Gout occurs when uric acid crystals form in joint spaces. Everyone has some level of uric acid in their blood stream. However, it is only when the level becomes high enough that uric acid leeches into the joint spaces and crystallizes. Once there, the crystals cause signifcant inflammationand the affected joint becomes painful, red, and swollen.
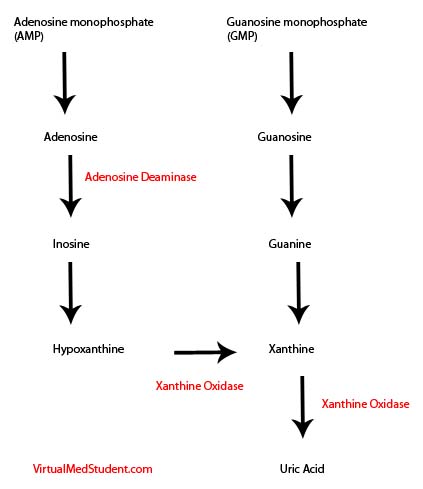
The causitive agent, uric acid, is a by product of purine catabolism. Purines are an important component of nucleotides, which are the building blocks of DNA and RNA. Purines are also seen in molecules like adenosine triphosphate, which serves as a source of cellular energy. The final product of the degradation of these molecules is, you guessed it, uric acid!
The degradation pathway for both adenine and guanine (and their constituent molecules) are shown below. The key enzymes involved in this degradation are shown in red.
When uric acid is formed, the kidneys filter it, and then excrete it into the urine. Some people are predisposed to either under-secrete or over-produce uric acid. In either case it builds up in the blood stream. This is known as "hyperuricemia". In some people hyperuricemia can cause gout. However, it is important to note that not everyone with hyperuricemia develops gout.
Diagnosis
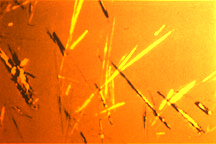
An official diagnosis of gout can only be made by tapping the joint (ie: sticking a needle into the joint and aspirating the contents) and looking at the fluid under a microscope.
If uric acid crystals are present, they will be "negatively birefringent", which means that they appear yellow under a parallel light source. Interestingly, if the light source is turned perpendicular the crystals turn blue (this is the exact opposite of pseudogout, which is discussed in another article).
Often times clinicians will order a blood uric acid test. In an acute attack, uric acid levels are meaningless because patients suffering from a gout flair may suprisingly have normal blood levels. However, in patients who are on medications to prevent gout, monitoring the blood uric acid levels can help guide treatment. In addition, hyperuricemia almost always precedes a gout attack.
Signs and Symptoms
As discussed above, the uric acid crystals cause inflammation in the joint space. This leads to a painful, swollen, and red joint. Gout attacks joints asymmetrically, meaning that it rarely affects the same joint on both sides of the body at that same time. Symmetric joint pain is more consistent with other rheumatological diseases.
Many joints can be affected by gout. The most common joint is the metatarsal phalangeal joint (MTP), which is a joint in the big toe. When this joint is involved the disease is referred to as "podagra".
Gout attacks usually occur quickly and unexpectedly with peaking of symptoms within 12 to 24 hours. Multiple repeated attacks of gout can lead to a chronic form of the disease known as "tophaceous gout". In chronic gout, not only are joints affected, but crystal formation can also occur in other areas of the body. For example, the achilles tendon and earlobes can be affected.

Patients with gout may also be at increased risk of developing uric acid kidney stones due to elevated uric acid in the urine.
Treatment
Acute treatment is aimed at controlling the inflammatory process within the joint. The most common drugs used to treat acute gout flairs are non-steroidal anti-inflammatory medications (NSAIDSs). Ibuprofen, naproxen, and indomethacin are the most common NSAIDs used to treat gout flairs. Steroids are also sometimes used, especially in people with contraindications to NSAIDs such as kidney failure.
An additional second line medication used to treat acute gout flairs is colchicine. It is typically used in people who cannot tolerate NSAIDs.
To prevent gout attacks from reoccurring, or to prevent tophaceous gout, there are several medicines that are used. The first medication is known as probenecid. It is most effective in people who "under-excrete" uric acid because it inhibits the re-absorption of uric acid in the kidney.
The second medication is known as allopurinol. It is most useful in people who "over-produce" uric acid because it inhibits the enzyme xanthine oxidase (see degradation pathway above) and reduces the amount of uric acid formed from the breakdown of purines.
Allopurinol and probenecid should not be used to treat acute gout flairs. Paradoxically, they can actually worsen an acute flair and should only be used to prevent recurrent attacks.
Overview
Gout is a disease of the joints caused by deposition of uric acid crystals. The joint becomes hot, swollen, red, and extremely painful. Diagnosis is made by aspiration of the crystals from the joint space. Treatment for acute flairs is usually with non-steroidal anti-inflammatories. Colchicine is occasionally used as well. Allopurinol and probenecid are used to prevent recurrent attacks.
References and Resources
- Bickley LS, Szilagyi PG. Bates’ Guide to Physical Examination and History Taking
. Ninth Edition. New York: Lippincott Williams and Wilkins, 2007.
- Kumar V, Abbas AK, Fausto N. Robbins and Cotran Pathologic Basis of Disease
. Seventh Edition. Philadelphia: Elsevier Saunders, 2004.
- Dalbeth N, So A. Hyperuricaemia and gout: state of the art and future perspectives. Ann Rheum Dis. 2010 Oct;69(10):1738-43.
- VanItallie TB. Gout: epitome of painful arthritis.Metabolism. 2010 Oct;59 Suppl 1:S32-6.
- Becker MA, Ruoff GE. What do I need to know about gout? J Fam Pract. 2010 Jun;59(6 Suppl):S1-8.