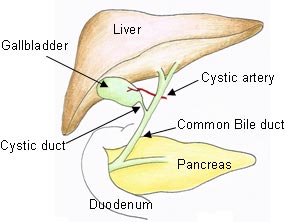
Gallstones (aka: cholelithiasis) are stones that form – you guessed it – in the gallbladder. In order to understand gallstones we have to understand how bile is formed. The gallbladder functions as a bile storage bin that releases its contents in response to signals from the intestine and stomach (ie: usually after a meal rich in fats). Bile is formed in the liver and is a unique mix of bile acids, cholesterol, bilirubin, water, phospholipids, and other electrolytes. The most important component is the bile acids. They help keep bile in its liquid state.
With a basic understanding of bile we can now address the problem of gallstone formation. There are different types of gallstones, and the most common type are cholesterol stones. When there is too much cholesterol in bile, the bile acids can no longer keep it soluble. The result? The excess cholesterol precipitates out and forms a stone.
The second type of gallstones are pigmented stones, which come in two flavors: brown and black. Brown stones form as a result of biliary tract infection. Black stones occur when the body breaks down red blood cells excessively, such as in hemolytic anemias. Black stones form from the excess bilirubin (a breakdown product of red blood cells), which gets sent to the liver and ultimately ends up in bile. An excessive amount will do exactly like cholesterol does, and precipitate to form a stone.
Signs and Symptoms
The common risk factors associated with gallstone formation are the “4 Fs”:
– Female
– Fat (overweight/obese, to use the politically "correct" term)
– Fertile
– Forty
Gallstones tend to develop in this demographic more often than in other people. Any one of these factors puts you at increased risk of developing gallstones. Other common risk factors include the following: oral contraceptive use, rapid weight loss, hemolytic diseases/disorders, small bowel resection, total parenteral nutrition (ie: nutrition given through an IV), Crohn’s disease, cystic fibrosis, and Native American ethnicity.
Gallstones by themselves are usually not symptomatic. In fact, many people are walking around with gallstones and don’t even know they have them! However, in a subset of the population symptoms develop. The main symptom associated with gallstones is biliary colic, which is pain that occurs after a meal (especially meals rich in fats). In addition, nausea, vomiting, and fatty food intolerances may also occur.
Complications
The second complication of gallstones is choledocholithiasis. This is a fancy term for a gallstone lodged in the common bile duct. This can lead to jaundice, pain, pancreatitis, and potentially a very dangerous condition known as acute cholangitis. Acute cholangitis is infection of the biliary tree and can occur secondary to an obstructing stone in the common bile duct.
To review, the common complications of gallstones are:
(1) Biliary colic
(2) Acute cholecystitis
(3) Choledocholithiasis
(4) Acute cholangitis
(5) Pancreatitis
Diagnosis
Since most gallstones are cholesterol, they are radiolucent, meaning that they are not detectable by x-rays. The test that is often done first with any suspected biliary pathology is a right upper quadrant ultrasound. If stones are present they will cast a “shadow” that can be picked up on the ultrasound. Often times additional studies are performed if another diagnosis is being considered. Some clinicians will get hepatitis studies to rule out liver damage. Pancreatic function is also commonly tested.
Treatment
Most gallstones do not require treatment because they are asymptomatic. However, if symptoms develop a trial of lifestyle modification is often tried. For example, avoiding fatty foods can limit biliary colic.
The definitive treatment for symptomatic gallstones, or if any of the complications above develop, is a cholecystectomy. Cholecystectomy is the medical term for removal of the gallbladder. It is done either "open" (ie: with a large incision) or laparoscopically depending on the patient and surgeon’s preferences.
Some patients may not be able to undergo surgery. In these patients a medication known as ursodiol may be given. It is a bile acid mimic that helps liquify bile.
Overview
Cholelithiasis (gallstones) is caused by precipitation of cholesterol or bilirubin. Gallstones are usually asymptomatic, although they can sometimes lead to biliary colic, acute cholecystitis, acute cholangitis, choledocholithiasis, and pancreatitis. Treatment, when symptomatic, is usually lifestyle modifications; if dangerous symptoms or complications occur treatment is with cholecystectomy (ie: removal of the gallbladder).
References and Resources
- Venneman NG, van Erpecum KJ. Pathogenesis of gallstones. Gastroenterol Clin North Am. 2010 Jun;39(2):171-83, vii.
- van Erpecum KJ. Biliary lipids, water and cholesterol gallstones. Biol Cell. 2005 Nov;97(11):815-22.
- Stinton LM, Myers RP, Shaffer EA. Epidemiology of gallstones. Gastroenterol Clin North Am. 2010 Jun;39(2):157-69, vii.
- Gurusamy KS, Davidson BR. Surgical treatment of gallstones. Gastroenterol Clin North Am. 2010 Jun;39(2):229-44, viii.
- O’Neill DE, Saunders MD. Endoscopic ultrasonography in diseases of the gallbladder. Gastroenterol Clin North Am. 2010 Jun;39(2):289-305, ix.
- Flynn JA. Oxford American Handbook of Clinical Medicine (Oxford American Handbooks of Medicine). First Edition. Oxford University Press, 2007.
- Kumar V, Abbas AK, Fausto N. Robbins and Cotran Pathologic Basis of Disease. Seventh Edition. Philadelphia: Elsevier Saunders, 2004.
- Blackbourne LH. Surgical Recall, North American Edition (Recall Series). Ninth Edition. Philadelphia: Lippincott Williams and Wilkins, 2009.