In order to understand what a pneumothorax is we have to first appreciate the anatomy of the lung and its surrounding tissues.
The lung is enveloped by two layers of connective tissue known as the visceral and parietal pleura. The visceral pleura is directly connected, and immediately adjacent to the lungs. The parietal pleura sits on top of the visceral pleura like a blanket, but is not, in the strictest sense of the word, attached to the visceral pleura.
This unique arrangement creates a potential space between the visceral and parietal layers. Normally this space is empty and the layers of pleura sit directly on top of one another. However, in some instances air can dissect into that potential space. When this occurs it is called a “pneumothorax”.
Classification
A pneumothorax is classified as either “simple” or “tension”. A tension pneumothorax occurs when a progressively larger amount of air gets trapped in the space between the parietal and visceral pleural layers.
Tension pneumothoraces occur when the pathology causing the pneumothorax creates a one way valve mechanism allowing air into, but not out of the pleural space. With each breath more air is drawn into the pneumothorax, but is unable to escape. The end result is progressive enlargement of the pneumothorax. As a result, the air pushes the heart and mediastinal structures to the opposite side of the chest. And this is no bueno.
On the other hand, a simple pneumothorax is present when the amount of air remains stable, and there is no shift of mediastinal structures.
Causes
Anything that introduces air between the parietal and visceral pleura can cause a pneumothorax. Trauma is a common cause of pneumothorax and can occur if the chest wall is damaged or a bronchus ruptures. Subpleural blebs, which are basically small “air blisters” on the surface of the lung are also common causes of non-traumatic pneumothorax. Patients who smoke, or who have underlying connective tissue diseases such as Marfan’s syndrome are at increased risk of developing a pneumothorax. For unclear reasons, spontaneous pneumothorax is often seen in tall, thin, white males.
Signs and Symptoms
Signs and symptoms are usually dependent on the size of the pneumothorax. One common symptom is “pleuritic” chest pain. This is caused by air irritating the parietal pleura; this type of pain is usually worse when the patient takes a breath. Patients also commonly complain of dyspnea (ie: shortness of breath).
On physical exam the patient will have decreased or absent breath sounds over the area of the pneumothorax. In addition, if you percuss (ie: tap) the patient’s lung with your finger it will sound hyper-resonant. In tension pneumothoraces the air may push on heart structures leading to tachycardia (ie: increased heart rate) and hypotension (ie: decreased blood pressure).
Diagnosis
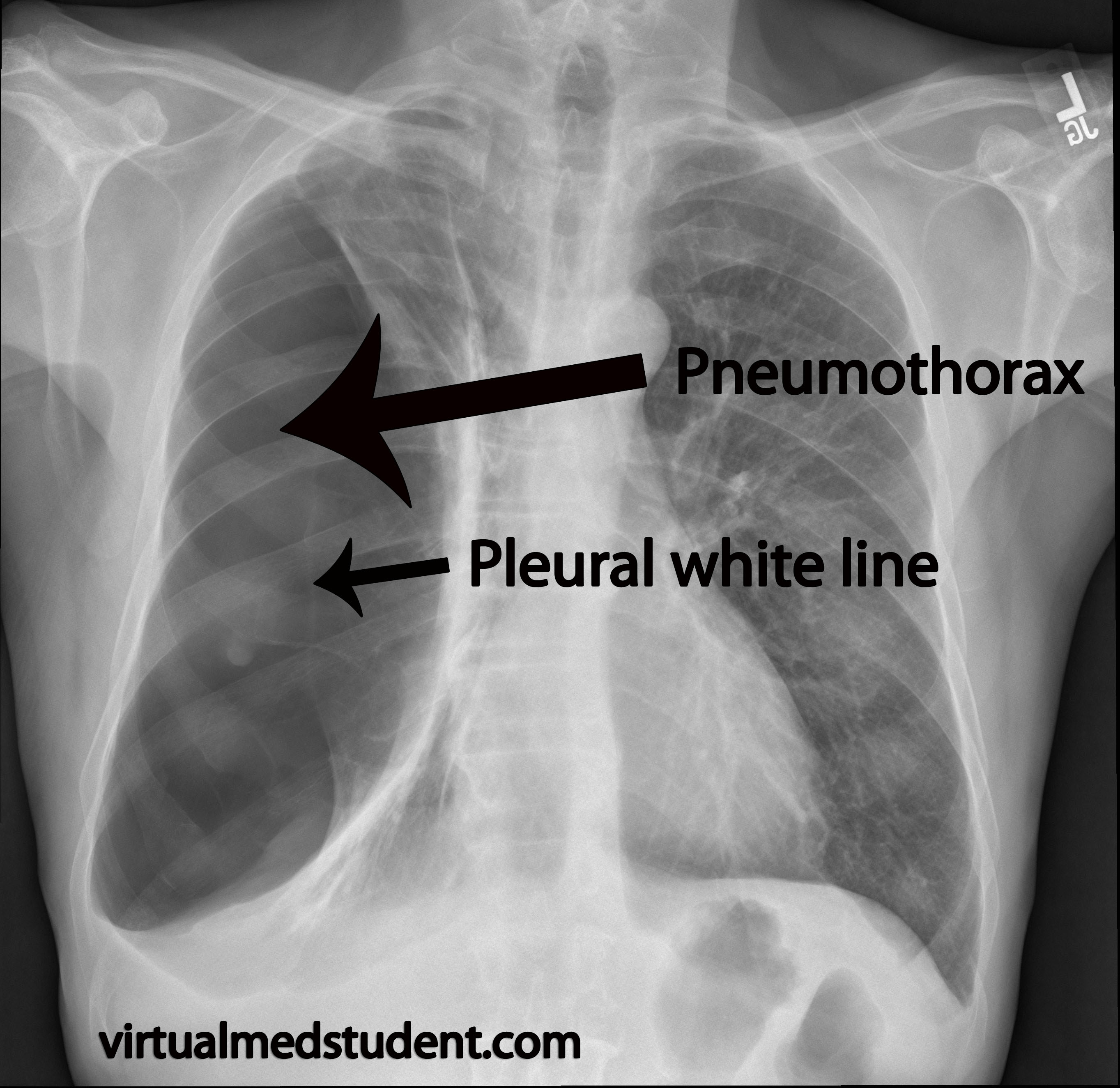
The first is absence of lung markings. However, this is not a fool proof system because lung markings may be absent in other diseases of the lung such as bullae. You also need to see a white line that parallels the chest wall. This is known as the "pleural white line", which represents separation of the visceral and parietal pleura. Additionally, in a tension pneumothorax the heart structures and trachea will deviate away from the pneumothorax.
Treatment
Treatment is dependent on the size of the pneumothorax and whether or not the patient has symptoms. Small (ie: less than 3cm between the chest wall and lung tissue) and asymptomatic lesions can be treated conservatively with supplemental oxygen via a nasal cannulae or face mask.
If the pneumothorax is larger than 3cm, or the patient has symptoms, a needle can be used to aspirate the air out of the chest. If this fails to re-inflate the lung, the patient will likely have to have a chest tube placed. In addition, any patient who is clinically unstable should have a chest tube placed.
Tension pneumothoraces are treated emergently by inserting a large bore needle into the 2nd intercostal space at the midclavicular line. This allows trapped air to escape through the newly created needle hole and prevents further air trapping.
Overview
A pneumothorax occurs when air dissects between the visceral and parietal pleural layers that envelope the lung. There are numerous causes. Symptoms include chest pain and shortness of breath although small pneumothoraces may be asymptomatic. Diagnosis is generally made from a chest x-ray. Treatment depends on symptomatology and the size of the pneumothorax.
References and Resources
- Pawloski DR, Broaddus KD. Pneumothorax: a review. J Am Anim Hosp Assoc. 2010 Nov-Dec;46(6):385-97.
- van Berkel V, Kuo E, Meyers BF. Pneumothorax, bullous disease, and emphysema. Surg Clin North Am. 2010 Oct;90(5):935-53.
- Luh SP. Review: Diagnosis and treatment of primary spontaneous pneumothorax. J Zhejiang Univ Sci B. 2010 Oct;11(10):735-44.
- Yadav K, Jalili M, Zehtabchi S. Management of traumatic occult pneumothorax. Resuscitation. 2010 Sep;81(9):1063-8.
- Simpson G. Spontaneous pneumothorax: time for some fresh air. Intern Med J. 2010 Mar;40(3):231-4.