Pathology
Aortic dissection occurs when blood flows into a “false” pathway created by damage to a layer of the aorta. In order to understand dissections, we have to first appreciate the layers of the aorta. Most blood vessels have three layers: the intima, media, and adventitia (see image below). You can think of these layers as insulation around a pipe. The adventitia is the outermost portion of the “pipe”; it helps connect the blood vessel to adjacent structures in the body. The media is the middle most layer, and is composed of smooth muscle; it helps control the diameter, and therefore pressure within the vessel. The intima is the layer that is immediately adjacent to blood flow.
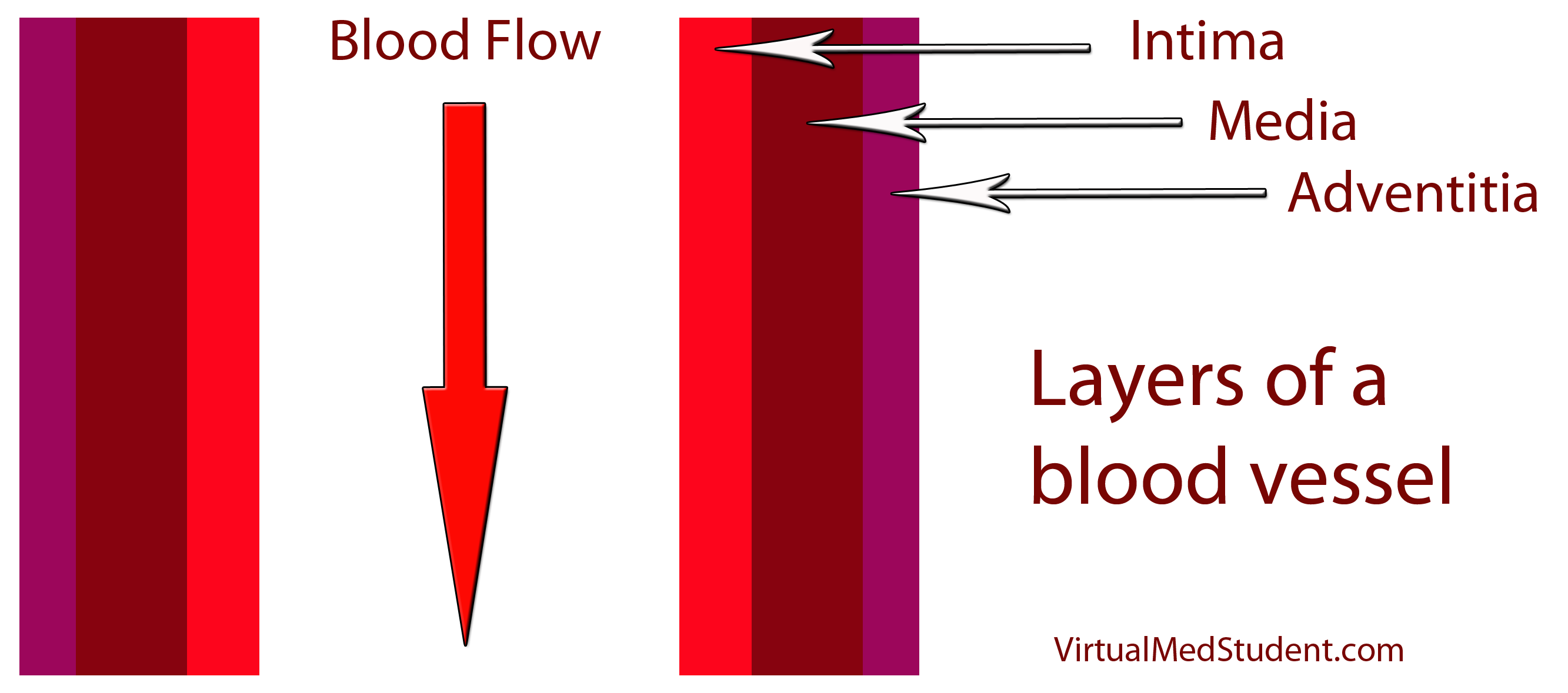
And this is precisely what happens in aortic dissection. The intimal layer of the vessel tears. As a result blood can now take one of two possible pathways:
(1) Down into the aorta (ie: its normal path).
(2) Into the “false” space between the intimal and medial layer (aka: a "false lumen").
If blood takes the later pathway it ultimately “dissects” the intimal and medial layer away from one another, hence the name aortic “dissection”. Ultimately, the classification and treatment of aortic dissections depends on where along the aorta the dissection occurs.
Classification Systems
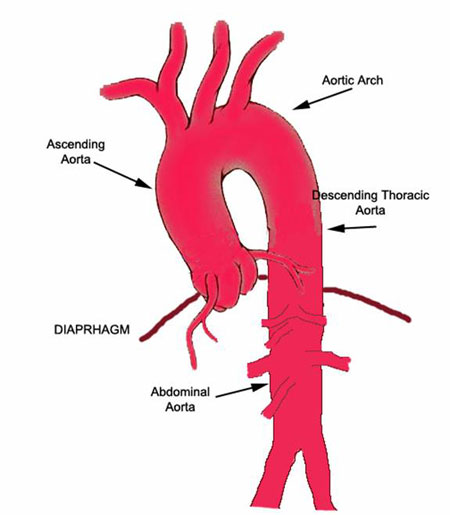
– DeBakey type 1 -> involves the ascending and descending aorta.
– DeBakey type 2 -> involves the ascending aorta only.
– DeBakey type 3 -> involves the descending aorta only.
The second classification system is more simple. It is called the Stanford classification, and is divided into 2 subtypes:
– Stanford type A -> Involves the ascending aorta (may or may not involve the descending aorta)
– Stanford type B -> involves the descending aorta (does not involve the ascending aorta)
The reason these classification systems exist is because the location of the dissection dictates treatment. Ascending dissections are treated much differently than descending dissections.
Signs and Symptoms
The symptoms of aortic dissection depend on its location. If the dissection affects the ascending aorta the classical presentation is a tearing or ripping chest pain. If the descending aorta is involved the pain is often referred to the upper back between the scapulae. In addition, patients usually come in with elevated blood pressures (which is usually the precipitating cause in most cases). However, the blood pressure readings can be different between arms. Pulses from blood vessels that originate before the dissection are often stronger. This can lead to pulse asymmetry on physical exam.
New heart murmurs can also occur. The most common one is the murmur of aortic regurgitation. New murmurs occur when the aortic root is involved in the dissection. This can cause mechanical damage to the aortic valve leading to abnormal function. Blood is then able to regurgitate (ie: flow backwards) into the heart due to the deficient valve.
Since the aortic arch (the portion between the ascending and descending sections) contains vessels that eventually go to the brain, patients sometimes have neurological symptoms as well, although this is a relatively uncommon finding in clinical practice.
Diagnosis
The diagnosis of aortic dissection is based on clinical suspicion combined with imaging studies. Chest x-ray will sometimes show a “widened mediastinum”. This occurs because the enlarged aorta casts a larger shadow on the x-ray detector. If this is seen, and there is a high clinical suspicion of a dissection, a CT scan of the chest with intravenous contrast is ordered (see image).
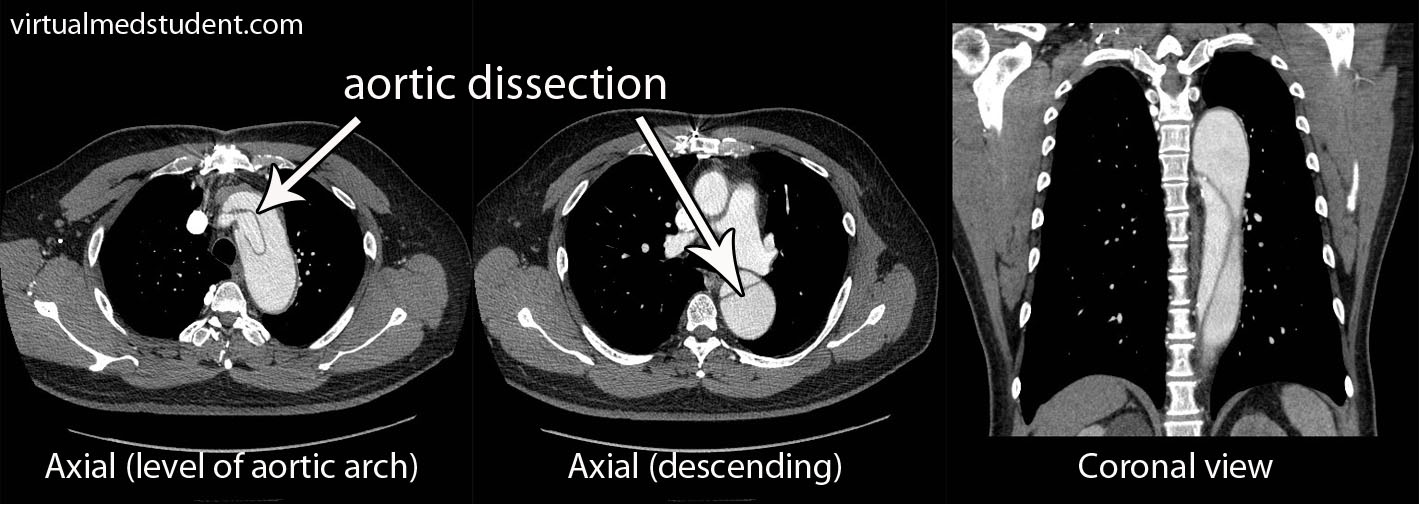
The CT scan will show the true and false lumens associated with dissection. Transesophageal echocardiography (TEE) is another way of visualizing the aorta and is highly sensitive and specific for detecting dissections.
Treatment
Treatment is dependent on the location of the dissection along the aorta. Dissections of the ascending aorta (DeBakey type 1 and 2, and Stanford class A) are surgical emergencies and require operative repair.
Descending aortic dissections (DeBakey type 3, and Stanford class B) are often managed medically through blood pressure control.
With the advent of endovascular techniques, many dissections can be treated endovascularly (ie: "through the groin"), which may be superior to open operative techniques for certain types of dissections.
Overview
Aortic dissections occur after damage to the intimal layer of the blood vessel. There are different classification systems depending on what part of the aorta is involved. Symptoms are usually a severe ripping chest pain that can radiate to the back. Pulses and blood pressures may vary between the right and left arms. In addition, neurological symptoms may occur if the dissections includes the vessels leading to the head. If the ascending aorta is involved surgery is indicated; descending aortic dissections are usually managed with aggressive blood pressure control.
References and Resources
- Kumar V, Abbas AK, Fausto N. Robbins and Cotran Pathologic Basis of Disease. Seventh Edition. Philadelphia: Elsevier Saunders, 2004.
- Lilly LS, et al. Pathophysiology of Heart Disease: A Collaborative Project of Medical Students and Faculty. Fourth Edition. Lippincott Williams and Wilkins, 2006.
- Flynn JA. Oxford American Handbook of Clinical Medicine (Oxford American Handbooks of Medicine). First Edition. Oxford University Press, 2007.
- Blackbourne LH. Surgical Recall, Fifth North American Edition (Recall Series). Fifth Edition. Philadelphia: Lippincott Williams and Wilkins, 2009.
- Hata M, Sezai A, Yoshitake I, et al. Clinical trends in optimal treatment strategy for type a acute aortic dissection. Ann Thorac Cardiovasc Surg. 2010 Aug;16(4):228-35.
- Nordon IM, Hinchliffe RJ, Loftus IM, et al. Management of Acute Aortic Syndrome and Chronic Aortic Dissection. Cardiovasc Intervent Radiol. 2010 Nov 12. [Epub ahead of print].