The spine is composed of thirty-three bony elements referred to as vertebrae. Each vertebrae connects with the vertebrae above and below it. These connection points are referred to as “facet” joints.
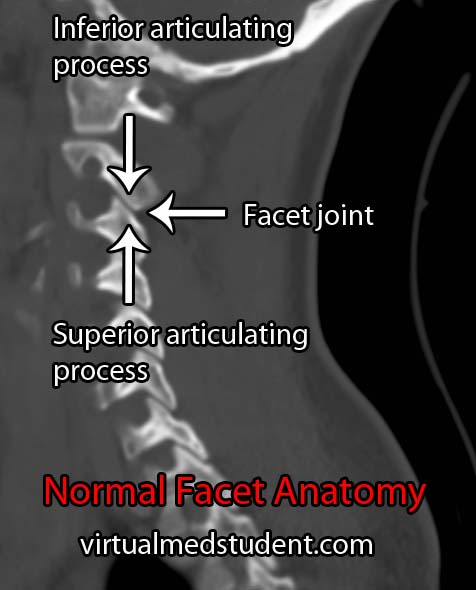
Each vertebrae has two bony sections known as superior articulating processes, as well as two bony sections known as inferior articulating processes. The inferior articulating processes of one vertebrae connect with the superior articulating processes of the vertebrae directly below it; the connections are held in place by ligaments.
The combination of the superior articulating process, inferior articulating process, and ligaments that connect them together form the facet joint. This arrangement makes the joints look like shingles on the roof of a house (see image below).
Like any other joint in the body, facet joints can dislocate. This is most likely to occur in the cervical spine where the facet joints are more horizontal in orientation.
Facet joint dislocations occur under conditions of severe flexion and/or rotation. The flexion injury causes disruption of the ligaments that stabilize the joint; this allows the inferior articulating process of the top vertebrae to "jump" over the superior articulating process of the bottom vertebrae. The end result is a dislocated (aka: "jumped" or "locked") facet.
Signs and Symptoms
Roughly a quarter of patients will have no signs or symptoms if one facet joint is dislocated between two vertebrae; another quarter will have incomplete spinal cord injuries. Ten percent will be paralyzed or paretic (ie: unable to move their arms or legs) and the remaining forty percent will have injury to the nerve roots exiting the spinal column. Nerve root injuries can cause paresthesias (ie: abnormal sensations) in a dermatomal pattern, as well as decreased reflexes and muscle weakness in the muscle group that the nerve serves.
The stakes for spinal cord injury increase dramatically if both facet joints are dislocated between two vertebrae. Roughly three quarters of these patients will be paralyzed! Very few people escape bilateral jumped facets without neurological injury.
Diagnosis
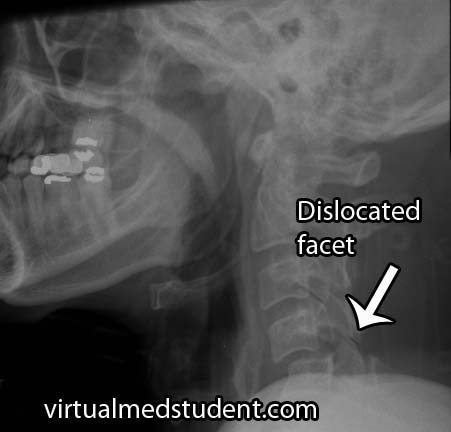
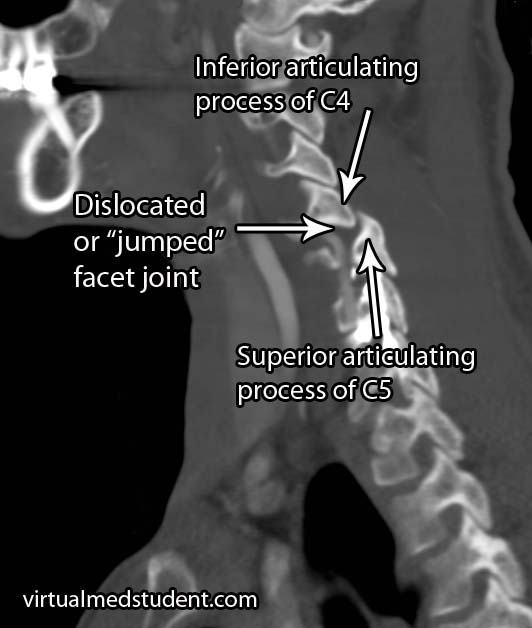
Diagnosis can be made with x-ray and CT imaging of the spine. The image will show the inferior articulating surface of the top vertebrae displaced anterior (ie: towards the chest) and inferior (ie: towards the feet) relative to the superior articulating surface of the bottom vertebrae.
The x-ray and CT scan to the right show a jumped facet between the fourth and fifth cervical vertebrae.
Treatment
Treatment of most facet dislocations begins with external traction. This involves placing tongs on the patient’s head and applying weight to gently distract (ie: pull apart) the spine.
Continuous x-rays are taken until the inferior articulating process of the dislocated joint is perched on top of the superior articulating process of the vertebrae below. At this point the weight is gradually reduced until the joint "pops" back into the proper anatomical position.
Since facet joint dislocations involve severe ligamentous injury, patients often require surgical intervention to stabilize the neck, even after reduction with external traction.
Overview
A dislocated facet joint occurs when the inferior articulating process of one vertebrae jumps over the superior articulating process of the vertebrae below it. This usually occurs after severe flexion and rotational injuries. Diagnosis is made on x-ray or CT of the spine. Treatment is usually with a combination of external traction and surgical fusion.
Related Articles
- Os odontoideum
- Atlas fractures
- Hangman’s fracture
- Odontoid fractures
- Ossified posterior longitudinal ligament
- Three column spine model
References and Resources
- Dvorak MF, Fisher CG, Fehlings MG, et al. The surgical approach to subaxial cervical spine injuries: an evidence-based algorithm based on the SLIC classification system. Spine (Phila Pa 1976). 2007 Nov 1;32(23):2620-9.
- Patel AA, Dailey A, Brodke DS, et al. Subaxial cervical spine trauma classification: the Subaxial Injury Classification system and case examples. Neurosurg Focus. 2008;25(5):E8.
- Rabb CH, Lopez J, Beauchamp K, et al. Unilateral cervical facet fractures with subluxation: injury patterns and treatment. J Spinal Disord Tech. 2007 Aug;20(6):416-22.
- Andreshak JL, Dekutoski MB. Management of unilateral facet dislocations: a review of the literature. Orthopedics. 1997 Oct;20(10):917-26.
- [No authors listed]. Treatment of subaxial cervical spinal injuries. Neurosurgery. 2002 Mar;50(3 Suppl):S156-65.
- Handbook of Neurosurgery
. Sixth Edition. New York: Thieme, 2006. Chapter 25.
- Baehr M, Frotscher M. Duus’ Topical Diagnosis in Neurology: Anatomy, Physiology, Signs, Symptoms
. Fourth Edition. Stuttgart: Thieme, 2005.